Does Retinol Thin Your Skin? The Science Behind Skincare's Scariest Myth
Understanding the two-layer reality — and why the answer depends entirely on which layer you're asking about
The Fear That Keeps People Off Retinol
Ask someone why they stopped using retinol — or why they never started — and “it thins your skin” comes up with surprising frequency. The concern is understandable: retinol can make skin look temporarily thinner, flakier, or more transparent early on, and the fear of long-term structural damage is enough to keep many people away from the most clinically-supported anti-aging ingredient in dermatology.
The claim is also wrong. And it’s wrong in a specific, scientifically interesting way that reveals exactly how retinol works.
Skin Has Two Distinct Layers — and They Respond Opposite Ways
Understanding the “does retinol thin skin” question requires separating skin into its two structurally and functionally different compartments.
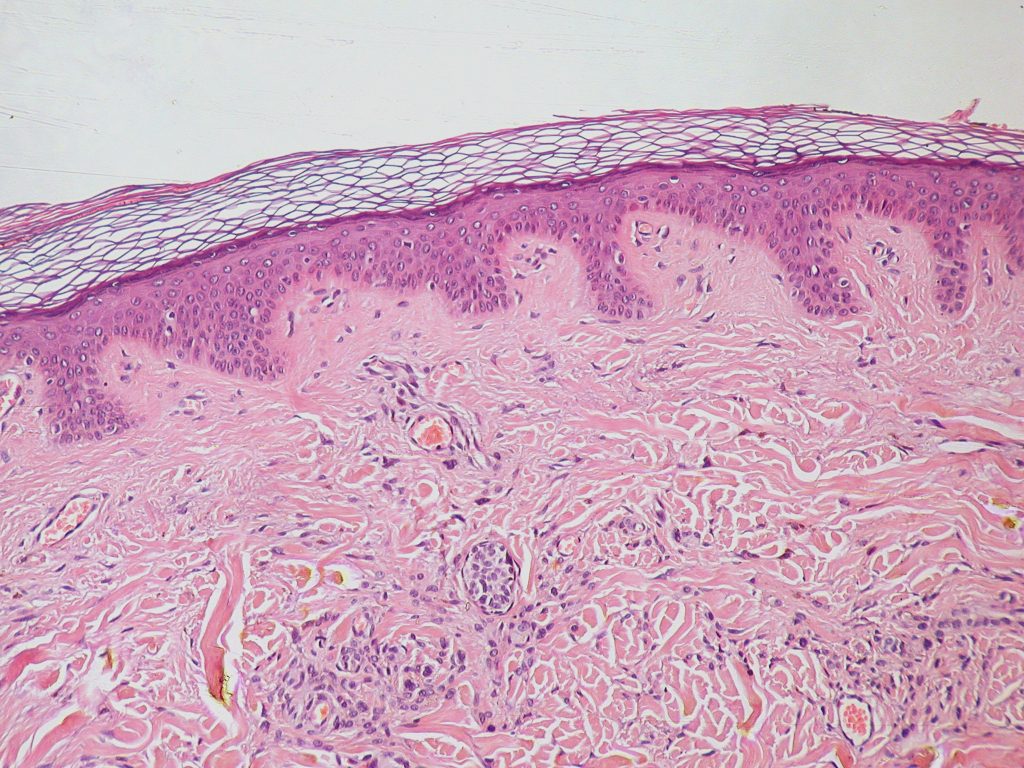
The stratum corneum is the outermost layer of the epidermis — a thin barrier of dead, flattened keratinocytes arranged like tiles on a roof. It’s the layer you can feel, the layer that gets rough and dull with age, and the layer that interacts directly with your environment. The stratum corneum thickens with age as the rate of desquamation (natural shedding) slows — dead cells accumulate and don’t shed as efficiently, creating a compacted, uneven surface.
The viable dermis sits beneath the epidermis and contains the structural proteins — collagen, elastin, fibronectin — that give skin its thickness, firmness, and bounce. This is the layer that actually determines whether your skin looks full and youthful or thin and saggy. Dermal thickness declines with age as collagen production falls and matrix metalloproteinases (MMPs) increase, accelerating collagen degradation [1].
Here’s what retinol actually does to each layer:
What Retinol Does to the Stratum Corneum: Controlled Thinning
Retinol accelerates the rate at which dead keratinocytes shed from the stratum corneum — a process called desquamation. The result is a thinner, more compact stratum corneum. If someone is measuring only this layer and calling it “skin thinning,” they’re technically correct about the number — but they’re describing the mechanism responsible for retinol’s most visible cosmetic benefits.
A thinner stratum corneum means:
- Smoother surface texture (less rough accumulation of dead cells)
- Brighter appearance (fresher, newer cells visible at the surface)
- Better ingredient penetration to the living cells below
- Reduced appearance of rough patches and uneven tone
This is the same outcome you’re seeking when you use an exfoliant. Retinol achieves it through a different mechanism — normalizing cell turnover at the keratinocyte level — rather than mechanically removing dead cells. Neither process constitutes harmful thinning of the skin.
Ask someone why they stopped using retinol — or why they never started — and “it thins your skin” comes up with surprising frequency.
What Retinol Does to the Viable Epidermis and Dermis: Structural Thickening
This is where the myth completely falls apart. Multiple independent clinical studies have measured retinol’s effects on the living layers of skin — and the consistent finding is net thickening, not thinning.
A comparative study by Kong et al. found that four weeks of topical retinol application significantly increased epidermal thickness by H&E staining and in vivo confocal microscopy, while also upregulating collagen type I (COL1A1) and collagen type III (COL3A1) gene expression with corresponding increases in procollagen I and procollagen III protein [1].
A study by Shao et al. examined the molecular basis of retinol’s anti-aging properties on naturally aged human skin in vivo, applying 0.4% retinol to sun-protected buttock skin of elderly subjects (76 ± 6 years old). The results were unambiguous: topical retinol “significantly increased epidermal thickness by stimulating keratinocyte proliferation and upregulation of c-Jun transcription factor” and simultaneously “significantly improved dermal extracellular matrix (ECM) microenvironment; increasing dermal vascularity by stimulating endothelial cell proliferation and ECM production (type I collagen, fibronectin and elastin) by activating dermal fibroblasts” [2]. This means retinol simultaneously:
- Increases keratinocyte proliferation → more new cells → thicker living epidermis
- Stimulates collagen I and III production → structurally thicker dermis
- Increases fibronectin and elastin → more resilient extracellular matrix
- Activates the TGF-β/CTGF pathway → the primary regulator of ECM homeostasis [2]
A 2022 study by Mellody et al. on photoaged skin confirmed this pattern: retinol “induced a stepwise increase in epidermal thickness” in a dose-dependent manner, and increased fibrillin-rich microfibril deposition (p < 0.01) — the scaffolding proteins essential for elastic tissue integrity [3].
The Keratinocyte Proliferation Finding Is Key
This point deserves special emphasis. Retinol increases keratinocyte proliferation — it stimulates the production of new skin cells. An ingredient that causes net cell thinning would do the opposite: reduce cell production or increase cell death. Retinol does neither.
What changes is the ratio of living to dead cells. The stratum corneum (dead layer) gets thinner because cells move through it faster. The viable epidermis (living layer) gets thicker because more new cells are being produced. The net effect on overall skin thickness — when you measure the whole structure — is an increase, not a decrease [1, 2, 3].
The Kafi et al. randomized controlled trial on naturally aged skin confirmed this: subjects using topical retinol showed significantly increased glycosaminoglycan expression in the dermis and measurable improvement in fine wrinkling compared to vehicle, consistent with increased dermal fullness and structural integrity [4].
Where the Myth Comes From
The perception of “thinning” likely originates from the retinoid adjustment period. During the first 4-8 weeks of retinol use, accelerated cell turnover temporarily outpaces the skin’s barrier repair mechanisms. The stratum corneum becomes temporarily thinner before it normalizes. Skin may look slightly more transparent or fragile during this window — which some people interpret as thinning.
During the first 4-8 weeks of retinol use, accelerated cell turnover temporarily outpaces the skin’s barrier repair mechanisms.
Sunburn sensitivity also increases during retinol use (another reason SPF is mandatory). Slightly pink, slightly sensitive, temporarily exfoliated skin looks and feels different. It’s not thinner in the structural sense — it’s a transient adjustment period that resolves as the skin adapts [5].
Does Long-Term Use Thin Skin?
This is perhaps the more concerning version of the question — not what retinol does initially, but whether decades of use cause cumulative thinning.
The evidence points the other way. The studies above measured outcomes after relatively short treatment periods (days to weeks). The long-term picture, supported by multiple clinical observations, is one of progressive collagen rebuilding and structural maintenance. Retinol’s mechanism — RAR nuclear receptor activation driving collagen gene transcription — doesn’t switch from “build” to “destroy” over time. The structural support being added accumulates with consistent use.
The critical qualifier: this holds for topical retinol and retinoids used as directed. Some historical concerns about skin thinning derived from high-dose systemic retinoids or misuse of prescription-strength tretinoin — a different clinical context entirely [5].
What Retinol Actually Does to Aging Skin
Skin aging is characterized by two processes happening simultaneously: the stratum corneum gets thicker (dead cell accumulation), while the dermis gets thinner (collagen and elastin loss) [5]. These are both forms of structural deterioration — dead cells piling up above, structural proteins breaking down below. Retinol reverses both trends simultaneously: it thins the compacted dead layer through normalized desquamation, and thickens the living dermis through collagen and keratinocyte stimulation. The net effect is skin that looks and structurally is more like younger skin — which is exactly what the clinical endpoint data show.
The myth isn’t just wrong. It gets the mechanism precisely backwards.
Delivery Determines How Much of This You Actually Get
The studies above used retinol concentrations of 0.1% to 0.4% in standard formulations applied under clinical conditions. Real-world retinol performance varies significantly based on delivery — conventional formulations lose significant potency to UV oxidation, alkaline pH instability, and poor barrier penetration before the retinol can reach the dermal fibroblasts where the structural work happens [5].
Nanoretinol® by North Biomedical® addresses this through lipid nanoparticle encapsulation. The biomimetic particles protect retinol from degradation en route and deliver it directly through the epithelial barrier to target cells — without the inflammatory trade-off that defines conventional retinol’s adjustment period. The result is +232% more collagen recovery compared to conventional retinol, with significantly reduced irritation during the adaptation phase.
The mechanism behind the clinical evidence is real. Getting the benefit requires a formulation that can actually deliver on it.
References
-
Kong R, Cui Y, Fisher GJ, et al. “A comparative study of the effects of retinol and retinoic acid on histological, molecular, and clinical properties of human skin.” J Cosmet Dermatol. 2016;15(1):49-57. doi:10.1111/jocd.12193
-
Shao Y, He T, Fisher GJ, Voorhees JJ, Quan T. “Molecular basis of retinol anti-ageing properties in naturally aged human skin in vivo.” Int J Cosmet Sci. 2017;39(1):56-65. doi:10.1111/ics.12348
-
Mellody KT, Bax DV, Roberts SA, et al. “Multifaceted amelioration of cutaneous photoageing by (0.3%) retinol.” Int J Cosmet Sci. 2022;44(6):625-635. doi:10.1111/ics.12799
-
Kafi R, Kwak HSR, Schumacher WE, et al. “Improvement of naturally aged skin with vitamin A (retinol).” Arch Dermatol. 2007;143(5):606-612. doi:10.1001/archderm.143.5.606
-
Quan T. “Human Skin Aging and the Anti-Aging Properties of Retinol.” Biomolecules. 2023;13(11):1614. doi:10.3390/biom13111614






