Collagen Banking: Why Your 40s Are the Best Time to Start
The science of building collagen reserves before menopause accelerates their loss
Think of collagen the way you think of a retirement account. You don’t start saving at 65 and expect a comfortable outcome. You build steadily during the decades when contributions are easiest and returns are highest — so that when the inevitable drawdowns begin, you have reserves to draw from.
That’s the premise of collagen banking, one of the most discussed shifts in anti-aging dermatology over the past two years. And the science behind it is more compelling than the trend cycle that gave it its name.
What Collagen Actually Does
Collagen is the structural protein that gives skin its firmness, bounce, and density. It’s the scaffolding inside the dermis that keeps everything in place. Type I and Type III collagen together account for roughly 80% of the skin’s dry weight, forming a dense matrix of fibers that holds moisture, supports elastin, and provides mechanical resistance to the forces that cause lines and sagging [1].
When that matrix is intact, skin snaps back. When it degrades — which happens continuously and irreversibly as we age — skin loses its resistance to deformation, thins, and eventually settles into the positions that gravity and repeated muscle movement encourage most.
The Production Timeline: When the Numbers Turn Against You
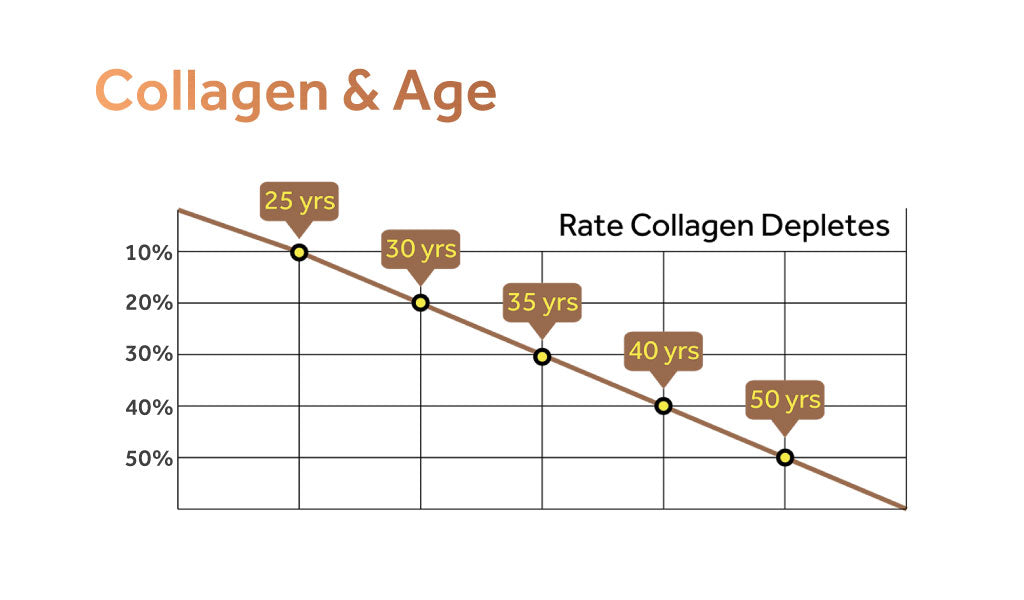
Collagen production peaks in the early-to-mid 20s and begins declining almost immediately after. Research by Varani and colleagues at the University of Michigan demonstrated that dermal fibroblasts from older skin produce measurably less type I procollagen than those from younger skin — a deficit driven both by cellular aging in the fibroblasts themselves and by the progressive fragmentation of the collagen matrix they sit within [1]. Fragmented collagen creates mechanical slack in the tissue, which reduces the tension that signals fibroblasts to keep producing. It becomes a self-reinforcing decline.
From age 25 onward, the net loss runs at roughly 1% per year under normal circumstances. That sounds slow until you consider what happens at menopause.
Estrogen plays a direct role in collagen synthesis, receptor expression, and the regulation of the enzymes (matrix metalloproteinases, or MMPs) that degrade collagen. When estrogen declines sharply at menopause, the balance tips hard. Studies have found that women lose approximately 30% of their skin’s total collagen content within the first five years after menopause [2], with annual reductions in collagen density of around 2.1% per year continuing through the postmenopausal period [3]. The same hormonal shift that transforms bone density trajectories is simultaneously remodeling the dermis.
From age 25 onward, the net loss runs at roughly 1% per year under normal circumstances.
For a woman who enters menopause at 51 with a depleted collagen reserve, this acceleration arrives at the worst possible time. For a woman who enters menopause at 51 with a dense, well-maintained matrix, the same rate of loss starts from a fundamentally stronger position.
That difference — the reserve you carry into the transition — is what collagen banking is designed to build.
The Banking Window
The most productive window for collagen banking is the decade or so before menopausal acceleration begins: roughly the late 30s through the mid-40s. During this period, estrogen levels are still relatively supportive, fibroblast function is declining but not yet severely compromised, and the collagen matrix still has enough structural integrity to respond meaningfully to stimulation. This is when topical interventions work best. The underlying machinery for collagen synthesis is still largely intact — it just needs consistent, evidence-based signals to stay active.
After menopause, the approach doesn’t become pointless — it just becomes harder and slower. You’re working against a stronger hormonal headwind. Starting earlier means you’re working with the biology that still favors a productive response.
The Tool Hierarchy: What Actually Stimulates Collagen
Skincare marketing has produced dozens of ingredients that claim to support collagen. Most of them work at the surface level — temporarily plumping the skin with hydration or filling the appearance of lines without touching the underlying architecture.
The evidence hierarchy looks like this:
Retinoids sit at the top, by a significant margin. A landmark 24-week clinical trial published in Archives of Dermatology demonstrated that topical retinol applied to naturally aged skin significantly increased both glycosaminoglycan expression and procollagen I immunostaining — the direct molecular building blocks of structural collagen — compared to a vehicle control [4]. The researchers specifically noted that retinol-treated aged skin showed greater capacity for matrix synthesis and wound response, which is a functional proxy for structural resilience.
This is not a moisturizing effect. It is a direct upregulation of the collagen synthesis pathway. Retinoids bind to nuclear retinoic acid receptors that regulate gene expression, activating the transcriptional programs that drive fibroblast activity and collagen production. A comprehensive review of retinoid clinical trials confirmed consistent improvements in collagen content, epidermal thickness, and skin matrix organization across multiple study designs [5].
The underlying machinery for collagen synthesis is still largely intact — it just needs consistent, evidence-based signals to stay active.
Peptides, vitamin C, and growth factors have supporting evidence but operate downstream and at lower effect sizes. They can be useful additions to a protocol, but for the primary task of driving collagen synthesis, no topical ingredient has the mechanistic depth or clinical evidence of retinoids.
Why Delivery Determines Results
Not all retinol reaches the dermis. This is the fundamental bottleneck that undermines most retinol products on the market.
Retinol must penetrate the stratum corneum and reach the deeper dermal layers where fibroblasts live to have any effect on collagen synthesis. Conventional retinol formulations face two obstacles: the epithelial barrier limits penetration, and many formulators compensate for this by using delivery vehicles that chemically disrupt the barrier — a method that causes the burning, peeling, and redness that makes many women abandon retinol entirely before it has a chance to work [5].
This trade-off — irritation in exchange for penetration — defines the experience most people associate with retinol. And it’s the reason compliance with conventional retinol is so poor in the demographic most likely to benefit from consistent use: women in perimenopause and menopause whose skin is already more reactive due to declining estrogen support.
A Smarter Delivery Architecture
Encapsulated retinol represents a different engineering approach to the same penetration problem. Rather than forcing entry through chemical disruption, lipid nanoparticle-encapsulated retinol is recognized by skin cells as biological “self” — the nanoparticle’s phospholipid membrane is structurally identical to cell membranes — and is transported through the barrier via natural cellular pathways.
Nanoretinol® is built on this technology. In head-to-head testing against conventional retinol, it demonstrated 232% greater effectiveness in collagen recovery and 73% greater effectiveness in elastin recovery. Clinical trials confirmed a 61% increase in skin firmness and a 56% increase in skin elasticity within 56 days of daily use — with significantly reduced cytotoxicity compared to standard retinol formulations.
For a collagen banking strategy, this combination matters: higher collagen stimulation with lower barrier disruption means you can maintain the consistent daily use that collagen building requires, without the cycles of irritation and recovery that interrupt conventional retinol regimens.
Starting the Practice
The key principles for using retinol as a collagen banking tool:
Start before you see the problem. The time to build reserves is before menopause accelerates loss. If you’re in your late 30s or 40s and your skin looks largely fine, that is not a reason to wait — it’s the ideal condition for preventive action.
Consistency beats intensity. A low concentration applied nightly over months and years builds more cumulative collagen than an aggressive concentration used intermittently. The fibroblast signaling that drives collagen synthesis responds to sustained exposure.
Pair with SPF every morning. UV radiation activates the matrix metalloproteinases that degrade collagen. Every unit of collagen produced overnight is vulnerable to UV degradation the following day if the skin is unprotected. Retinol and SPF are inseparable in any serious collagen banking protocol.
Set realistic timelines. Significant collagen remodeling takes months, not weeks. The trial data supporting retinol’s collagen effects used protocols of 24 weeks or longer. This is not a product that transforms skin in 30 days — it’s an investment that compounds over time, which is precisely what banking is designed to capture.
References
- Varani J, Dame MK, Rittie L, et al. “Decreased Collagen Production in Chronologically Aged Skin.” Am J Pathol. 2006;168(6):1861-1868. doi:10.2353/ajpath.2006.051302
- Castelo-Branco C, Duran M, González-Merlo J. “Skin collagen changes related to age and hormone replacement therapy.” Maturitas. 1992;15(3):197-207. doi:10.1016/0378-5122(92)90245-y
- Bravo B, Penedo L, Carvalho R, et al. “Dermatological Changes during Menopause and HRT: What to Expect?” Cosmetics. 2024;11(1):9. doi:10.3390/cosmetics11010009
- Kafi R, Kwak HSR, Schumacher WE, et al. “Improvement of Naturally Aged Skin With Vitamin A (Retinol).” Arch Dermatol. 2007;143(5):606-612. doi:10.1001/archderm.143.5.606
- Mukherjee S, Date A, Patravale V, Korting HC, Roeder A, Weindl G. “Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety.” Clin Interv Aging. 2006;1(4):327-348. doi:10.2147/ciia.2006.1.4.327






