Red Light Therapy for Wrinkles: What the Science Actually Says
Separating the peer-reviewed evidence from the marketing hype around photobiomodulation for skin aging
The Promise Behind the Red Glow
Walk into any beauty retailer or scroll through skincare social media, and you will encounter red light therapy devices promising to erase wrinkles, restore collagen, and reverse years of aging. LED masks, handheld wands, and full-panel systems are selling at unprecedented rates. But behind the glowing marketing materials lies a more nuanced scientific story — one that is genuinely encouraging, but also more complicated than most brands would like you to believe.
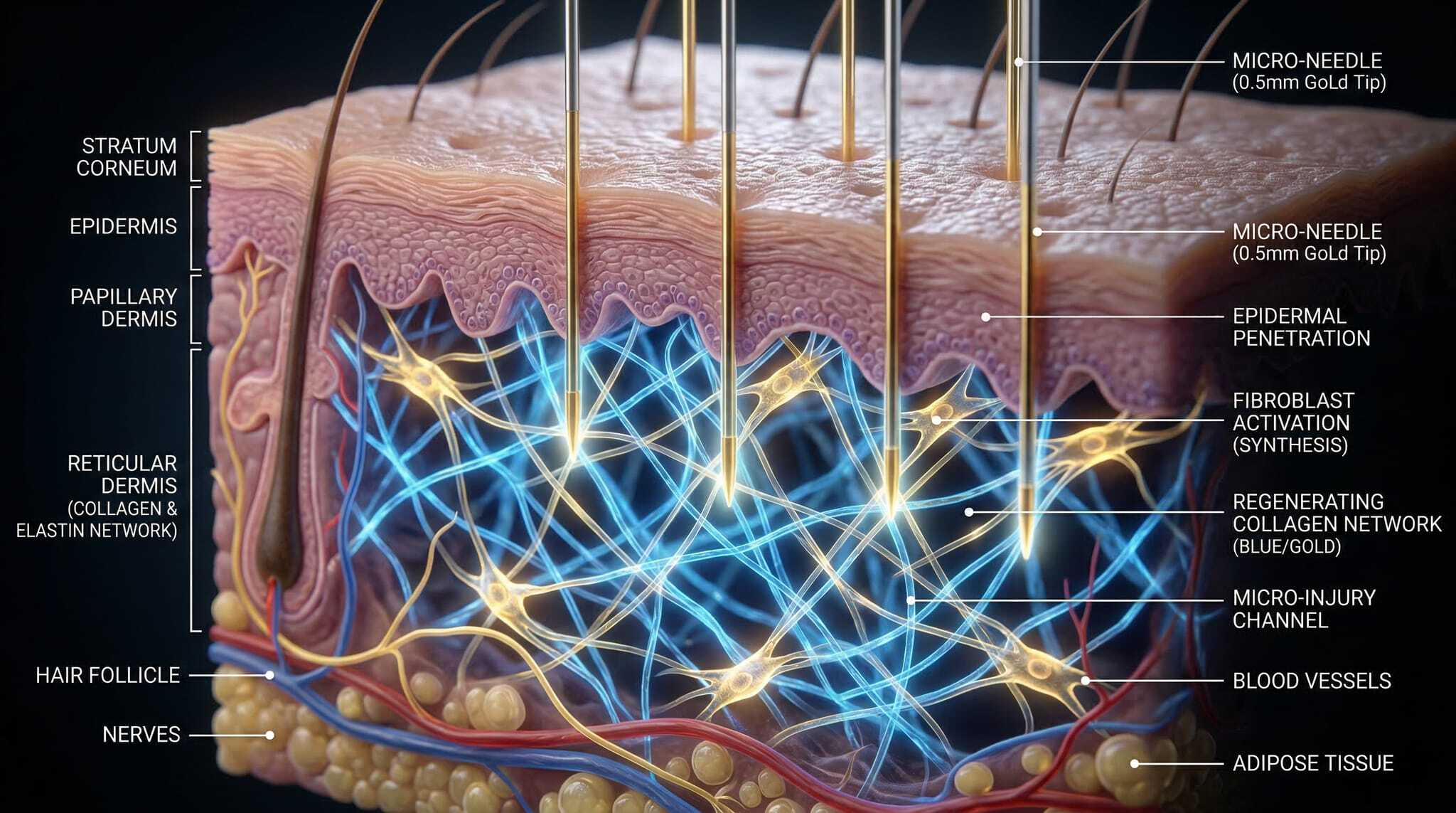
Red light therapy, technically known as photobiomodulation (PBM), uses specific wavelengths of visible and near-infrared light — typically between 620 and 850 nanometers — to influence cellular behavior without generating heat or causing tissue damage [1]. Unlike UV radiation, which accelerates photoaging, red and near-infrared light penetrate the skin to reach dermal fibroblasts — the cells directly responsible for producing collagen and elastin.
The question is not whether red light does something to skin cells. It clearly does. The real question is whether it does enough to meaningfully reduce wrinkles in real-world conditions.
How Red Light Talks to Your Cells
The mechanism behind photobiomodulation begins at the mitochondria. Cytochrome c oxidase, a photosensitive enzyme in the mitochondrial electron transport chain, absorbs photons in the red and near-infrared spectrum. When these photons reach the enzyme, they dissociate inhibitory nitric oxide molecules from its binding sites, effectively removing a metabolic brake [2].
The downstream effects cascade from there. Mitochondrial membrane potential increases. ATP production rises. Reactive oxygen species are generated at low, signaling-appropriate levels. These signals activate transcription factors — including NF-κB and AP-1 — that upregulate genes involved in cell proliferation, migration, and importantly, collagen synthesis [2].
Think of it like clearing a clogged fuel line in an engine. The machinery was always there; the light simply removes the obstruction and lets the cell run at full capacity again.
In a separate single-blinded study, Barolet and colleagues demonstrated that pulsed 660 nm LED treatment produced a 31% increase in type-1 procollagen production in tissue-engineered human skin models.
What the Clinical Trials Show
The most rigorous published trial on red light therapy for wrinkles remains the 2014 randomized controlled study by Wunsch and Matuschka, involving 136 volunteers split across treatment and control groups. Subjects received twice-weekly sessions of polychromatic red light (611–650 nm) over 30 sessions. The results were statistically significant: treated subjects showed measurably improved skin roughness, increased intradermal collagen density on ultrasound, and visible wrinkle reduction confirmed by blinded clinical photography assessment [1].
In a separate single-blinded study, Barolet and colleagues demonstrated that pulsed 660 nm LED treatment produced a 31% increase in type-1 procollagen production in tissue-engineered human skin models. When the protocol was then applied to aged and photoaged human subjects, over 90% showed measurable reduction in wrinkle depth, and 87% improved on the Fitzpatrick wrinkling severity score after just 12 treatments [3].
At the cellular level, research has shown that 660 nm light stimulates fibroblast differentiation — the process by which resting fibroblasts transform into active, collagen-secreting myofibroblasts [4]. This is particularly relevant for aging skin, where fibroblast activity naturally declines with each passing decade.
The Wavelength Question
Not all red light is created equal. The therapeutic window for skin rejuvenation falls primarily between 620 and 700 nm for superficial collagen stimulation, and 780 to 850 nm for deeper tissue penetration [5]. Consumer devices vary enormously in wavelength precision, power output, and treatment area — which means results from clinical trials using medical-grade equipment do not automatically translate to every at-home mask on the market.
Power density matters as much as wavelength. Clinical trials typically deliver 4 to 10 J/cm² per session. Many consumer devices fall below this threshold, which may explain why some users see minimal results despite consistent use. The relationship between dose and response follows a biphasic curve: too little light produces no effect, the optimal range produces cellular stimulation, and too much can actually inhibit the very processes you are trying to activate [5].
What Red Light Can and Cannot Do
Based on the current evidence, here is where red light therapy stands:
The honest summary: red light therapy is a genuinely promising, non-invasive complement to a comprehensive anti-aging routine — not a standalone replacement for proven topical actives like retinol.
Supported by clinical evidence:
- Increasing intradermal collagen density
- Reducing fine lines and surface roughness
- Improving overall skin texture and complexion
- Stimulating fibroblast activity and procollagen production
Not yet well-supported or overstated:
- Eliminating deep, set-in wrinkles (moderate improvement is more realistic)
- Replacing topical anti-aging actives entirely
- Producing permanent results without ongoing treatment
- Working at any wavelength, power, or device quality
The honest summary: red light therapy is a genuinely promising, non-invasive complement to a comprehensive anti-aging routine — not a standalone replacement for proven topical actives like retinol.
Combining Light Therapy with Topical Actives
Where red light therapy becomes most interesting is in combination protocols. Photobiomodulation stimulates collagen production from the mitochondrial level up, while topical retinoids work through a completely different pathway — binding nuclear retinoic acid receptors to upregulate collagen gene transcription and accelerate cell turnover.
These two mechanisms do not compete. They complement each other.
The same fibroblasts that red light activates are the ones that retinol instructs to produce more collagen. A fibroblast that is both metabolically energized (by light) and genetically instructed (by retinol) has every reason to outperform one receiving only a single signal.
For women over 40 dealing with the accelerated collagen loss that accompanies perimenopause and menopause, this dual-signal approach makes biological sense. Nanoretinol® takes this further by using biomimetic lipid nanoparticles to deliver retinol directly through the epithelial barrier — bypassing the harsh chemical penetration enhancers that make traditional retinol formulations irritating. The result is 232% more effective collagen recovery compared to conventional retinol [6], which means the retinol signal arriving at your fibroblasts is substantially stronger to begin with.
Pairing a well-designed red light device with an advanced delivery system like Nanoretinol® creates what amounts to a two-front strategy: light from the outside energizing your cells, and encapsulated retinol from the surface instructing them to rebuild.
The Practical Takeaway
Red light therapy for wrinkles is not a gimmick — the peer-reviewed evidence supports real, measurable benefits in collagen density and wrinkle reduction. But it is also not the miracle cure that marketing materials suggest. Results depend heavily on device quality, wavelength accuracy, power density, and consistency of use.
The strongest anti-aging strategy is rarely a single intervention. It is the intelligent combination of complementary approaches: sun protection, proven topical actives, and now, increasingly, photobiomodulation. The science supports each piece individually — and suggests they work better together.
References
- Wunsch A, Matuschka K. “A Controlled Trial to Determine the Efficacy of Red and Near-Infrared Light Treatment in Patient Satisfaction, Reduction of Fine Lines, Wrinkles, Skin Roughness, and Intradermal Collagen Density Increase.” Photomedicine and Laser Surgery. 2014;32(2):93-100. doi:10.1089/pho.2013.3616
- de Freitas LF, Hamblin MR. “Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy.” IEEE Journal of Selected Topics in Quantum Electronics. 2016;22(3):7000417. doi:10.1109/JSTQE.2016.2561201
- Barolet D, Roberge CJ, Auger FA, Boucher A, Germain L. “Regulation of Skin Collagen Metabolism In Vitro Using a Pulsed 660 nm LED Light Source: Clinical Correlation with a Single-Blinded Study.” Journal of Investigative Dermatology. 2009;129(12):2751-2759. doi:10.1038/jid.2009.186
- Mokoena DR, Houreld NN, Dhilip Kumar SS, Abrahamse H. “Photobiomodulation at 660 nm Stimulates Fibroblast Differentiation.” Lasers in Surgery and Medicine. 2020;52(7):671-681. doi:10.1002/lsm.23204
- Karu TI. “Mitochondrial Signaling in Mammalian Cells Activated by Red and Near-IR Radiation.” Photochemistry and Photobiology. 2008;84(5):1091-1099. doi:10.1111/j.1751-1097.2008.00394.x
- North Biomedical LLC. “Nanoretinol® vs. Conventional Retinol: Efficacy in Collagen and Elastin Recovery.” Clinical Study Summary, 2024.